
April 25th, 2023
Written by: Kara McGaughey
You probably heard about monoclonal antibodies during the COVID-19 pandemic. In November of 2020, the Food and Drug Administration (FDA) provided an emergency use authorization for Regneron’s monoclonal antibody as a COVID-19 treatment [1]. The intravenous (IV) drug cocktail quickly made its way into arms around the country, treating people, including former President Donald Trump, with coronavirus infections. However, monoclonal antibodies don’t just work for COVID-19. Since 2021, the FDA has given accelerated approval to two monoclonal antibodies designed to treat Alzheimer’s disease.
Here, we’ll explore how these monoclonal antibodies work, how effective they are, and how they’re shaping future Alzheimer’s disease research and drug development.
What exactly is a monoclonal antibody?
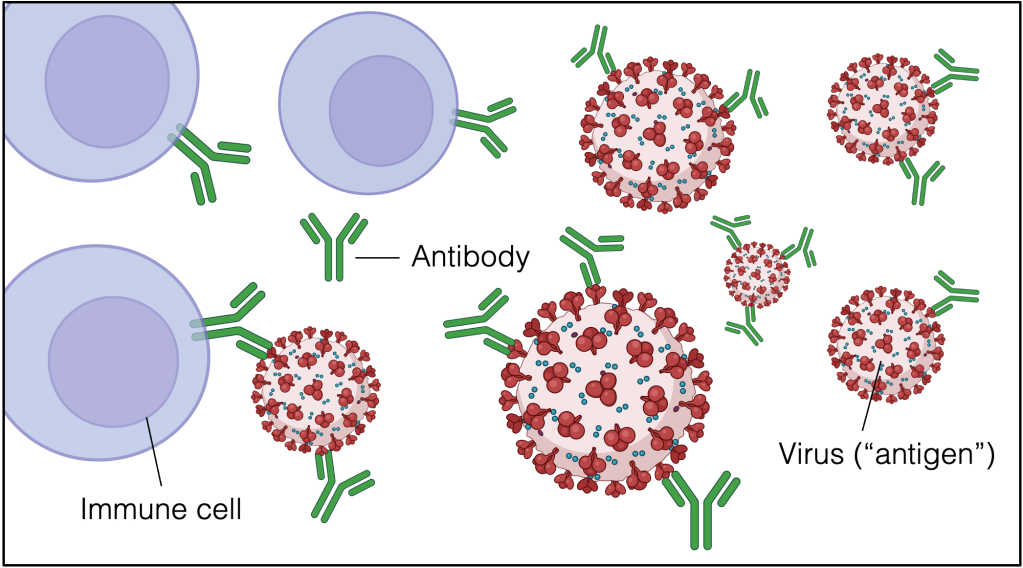
Antibodies are large, y-shaped proteins that your body uses to identify foreign objects (called “antigens”), like viruses, and flag them for your immune system to destroy [2]. Monoclonal antibodies are made in the lab, but designed to find and flag a particular antigen just like the antibodies your body makes naturally. Scientists can design monoclonal antibodies to bind all kinds of antigen targets. Regeneron’s monoclonal antibody, for example, binds spike proteins on the SARS-CoV-2 virus (Fig. 1). Once a monoclonal antibody binds its antigen target, it starts to signal to immune cells in the area, calling them over to break down and clean up what it’s found in order to keep you healthy.
Monoclonal antibodies aren’t new kids on the block. They have been playing a major role in medicine — both diagnosis and treatment — long before COVID-19. For example, many pregnancy tests work by using monoclonal antibodies to bind the hormone HCG, which is only found in the urine of pregnant people [3]. If HCG is present in the urine, it will stick to monoclonal antibodies on the test and trigger a change in color to indicate pregnancy. These tiny therapeutic agents have also been deployed to bind and destroy a wide variety of cancer cells from lung cancer to melanoma and lymphoma [4]. Most recently, monoclonal antibodies have been used to target and treat diseases, like Alzheimer’s.
How can we use monoclonal antibodies to treat Alzheimer’s disease?
Alzheimer’s is a neurodegenerative disease and the most common cause of dementia [5]. It is progressive, moving from mild memory loss to severe cognitive and physical impairments that leave patients requiring around-the-clock care. Part of what makes Alzheimer’s so tricky to diagnose and so debilitating for patients and their families is that by the time people begin showing signs of memory loss, the disease has already spread throughout the brain.
β-amyloid plaques are one feature of Alzheimer’s disease that accumulate and spread throughout the brain [6]. These plaques are formed when β-amyloid, a peptide our brains make naturally, fails to get broken down. Instead of being removed and recycled, β-amyloid peptides begin to stick to each other, eventually forming large β-amyloid plaques. The formation of these plaques has consequences. For decades, researchers have thought that β-amyloid plaques are the driving force behind Alzheimer’s disease [7]. In fact, every genetic mutation known to cause Alzheimer’s affects β-amyloid plaque formation [8].
So, finding a way to target and remove β-amyloid plaques should have a big effect on Alzheimer’s disease, and monoclonal antibodies provide exactly that opportunity. Instead of Regeneron’s drug that binds SARS-CoV-2 spike proteins, Alzhiemer’s disease monoclonal antibodies target β-amyloid and usher in the immune system to help with plaque breakdown. Since plaque accumulation begins before people experience changes in memory or cognitive functioning, a monoclonal antibody targeting β-amyloid could slow, or even stop, the progression of Alzheimer’s disease before it interferes with daily life. With no existing cure for Alzheimer’s, this would be a big deal for patients and their families. Before monoclonal antibodies, FDA-approved Alzheimer’s drugs aimed only to manage symptoms, keeping patients comfortable as the disease progressed. Monoclonal antibodies are the field’s first attempt to target the brain changes underlying Alzheimer’s disease itself.
There are currently two FDA-approved Alzheimer’s disease monoclonal antibodies, Aducanumab and Lecanemab, each designed to bind a different antigen. Aducanumab, approved by the FDA in 2021, is designed to find and flag accumulated β-amyloid plaques [9]. Lecanemab, which received FDA approval in January of 2023, takes a different approach, getting at Alzheimer’s disease pathology even earlier by targeting free-floating β-amyloid peptides before they have the chance to accumulate into plaques [10].
Do monoclonal antibodies work as an Alzheimer’s disease treatment?
In short, monoclonal antibodies for Alzheimer’s disease come with both success and failure.
Aducanumab and Lecanemab were tested on patients with early-stage Alzheimer’s disease whose brain scans showed β-amyloid accumulation. In both clinical trials, these patients were randomly assigned to receive an IV infusion of either the monoclonal antibody drug or a placebo. Regardless of which group they were in, all participants went through several rounds of cognitive testing (to track brain functioning) and PET imaging brain scans (to measure the amount of β-amyloid).
These PET scans showed something truly remarkable: The brains of patients who received monoclonal antibodies showed reduced levels of β-amyloid. However, despite this major molecular feat, neither drug had an effect on cognitive functioning large enough to be noticed or appreciated by Alzheimer’s disease patients and their families. In other words, while monoclonal antibodies have made it possible to flag and degrade β-amyloid using the body’s own immune system, the payoff wasn’t quite as big as expected, and patients in both drug and placebo groups continued to experience cognitive decline. Moreover, serious side effects, like swelling and bleeding in the brain, were relatively common [11].
Where do we go from here?
With monoclonal antibodies, we can finally target β-amyloid, which has been the primary focus of Alzheimer’s treatment research for the past three decades [7]. However, reducing β-amyloid doesn’t seem as effective as we hoped.
As such, many in the field are calling for Alzheimer’s disease research to consider new directions, moving away from β-amyloid and exploring other potential disease causes and treatment targets. Fortunately, there is no shortage of options! Not only are there other proteins that malfunction or accumulate during Alzheimer’s disease, but our growing understanding of how brain function relates to what’s going on with the rest of the body points fingers at things like communication with gut microbes and viral infections (which you can explore in this previous PNK post). Recent evidence also highlights inflammation and immune dysregulation as big contributors to Alzheimer’s and likely targets for therapy.
So, while the first two attempts at using β-amyloid-targeted monoclonal antibodies to treat Alzheimer’s disease have fallen short, there are plenty of other targets to be tried and these designer drugs are a technology that’s likely not going anywhere any time soon.
Interested in reading more? Check out our PNK archives for additional information on β-amyloid plaques and other potential Alzheimer’s disease drug targets, like ApoE.
References
[1] U.S. Food and Drug Administration. (2022). Fact sheet for health care providers Emergency Use Authorization (EUA) of Regen-COV. Retrieved from: https://www.fda.gov/media/145611/download.
[2] Nicholson, L.B. (2016). The immune system. Essays in Biochemistry, 60, 275-301. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5091071/.
[3] Carter, D. (2020). Monoclonal antibodies and cancer treatment: What to know. The University of Texas MD Anderson Cancer Center.
[4] Bluestein, D. (1988). Monoclonal antibody pregnancy tests. American Academy of Family Physicians, 38, 197-204. https://pubmed.ncbi.nlm.nih.gov/3394606/.
[5] Alzheimer’s Association. 2023 Alzheimer’s Disease Facts and Figures. Alzheimers Dementia, 19(4). https://doi.org/10.1002/alz.13016.
[6] Ballard, C., Gauthier, S., Corbett, A., Brayne, C., Aarsland, D. & Jones, E. (2011). Alzheimer’s disease. The Lancet, 9770, 1019-1031. https://doi.org/10.1016/S0140-6736(10)61349-9.
[7] Selkoe, D.J. & Hardy, J. (2016). The amyloid hypothesis of Alzhiemer’s disease at 25 years. EMBO Molecular Medicine, 8, 595-608. https://doi.org/10.15252/emmm.201606210.
[8] Bettens, K., Sleegers, K. & Van Broeckhoven, C. (2013). Genetic insights into Alzheimer’s disease. The Lancet Neurology, 12, 92-104. https://doi.org/10.1016/S1474-4422(12)70259-4.
[9] Beshir, S.A., Aadithsoorya, A.M., Parveen, A., Goh, S.S.L., Hussain, N. & Menon, V.B. (2022). Aducanumab therapy to treat Alzheimer’s disease: A narrative review. https://doi.org/10.1155%2F2022%2F9343514.
[10] van Dyck, C.H., Swanson, C.J., Aisen, P., Bateman, R.J., Chen, C., Gee, M., Kanekiyo, M., Li, D., Reyderman, L., Cohen, S., Froelich, L., Katayama, S., Sabbagh, M., Vellas, B., Watson, D., Dhadda, S., Irizarry, M., Kramer, L.D. & Iwatsubo, T. (2023). Lecanemab in early Alzheimer’s disease. New England Journal of Medicine, 388, 9-21. https://doi.org/10.1056/nejmoa2212948.
[11] Reardon, S. (2023). FDA approves Alzheimer’s drug Lecanemab amid safety concerns. Nature News. Retrieved from: https://www.nature.com/articles/d41586-023-00030-3.
Cover Photo by Diana Polekhina on Unsplash
Figure 1 made in BioRender.com by Kara McGaughey

Leave a comment