
April 9, 2019
Written by: Nitsan Goldstein
Imagine being able to change your mood within milliseconds with the switch of a button on a remote control. Sound like science fiction? You’re not entirely wrong! Scientists can alter brain activity and treat several neurological and psychiatric conditions using a technology called deep brain stimulation (DBS). The catch? No one is entirely sure why it works. In this post we’ll discuss the history of DBS, how scientists think it might be working, and how it is used today.
30 Years of DBS
Deep brain stimulation was first used as an experimental treatment for Parkinson’s disease. In Parkinson’s disease, neurons in a region of the brain called the basal ganglia and that release a chemical called dopamine degenerate. The basal ganglia is critical in the control of movement; instructing your muscles when to move and when to not move. The loss of these neurons is what causes patients with Parkinson’s to have trouble initiating movements and to suffer from tremors. Interestingly though, in the 1930s, neurosurgeons noticed that lesions, or targeted destruction, of parts of the basal ganglia actually improved tremors in patients with Parkinson’s1. Thus, ablative therapy became the only available treatment for Parkinson’s disease symptoms. Until, that is, the introduction of levodopa.
Levodopa is a drug that boosts the amount of dopamine to compensate for the dopamine that is lost when the neurons begin degenerating. The success of levodopa temporarily halted surgery as a treatment for Parkinson’s Disease1. However, it soon became clear that not only can levodopa cause serious side effects, the disease will still progress to a point where drug therapy is no longer effective. With renewed interest in surgical treatments for Parkinson’s disease as well as advancements in targeted electrical stimulation of brain structures, neurosurgeons began experimenting with DBS to treat Parkinson’s in the late 1980s1.
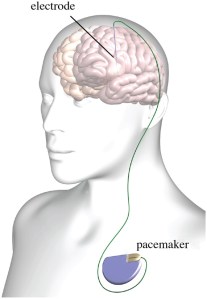
DBS involves placing electrical leads into specific regions of the brain to stimulate neural networks in those areas (Figure 1). They found that, incredibly, DBS in certain regions of the basal ganglia was as effective in treating Parkinson’s symptoms as ablative therapy (watch as a deep brain stimulator helps treat a man’s tremors caused by Parkinson’s Disease here). Additionally, DBS allowed for much more refined control of the levels and patterns of stimulation. If you’re thinking “wait… stimulating a brain region and destroying a brain region have the same effects? That doesn’t make sense!” then you are right, and scientists are still not sure why DBS is effective. Using animal models and other experimental strategies, however, there are a few theories as to how DBS might be working.
How might it be working?
DBS is a fascinating case in which scientists experimented with a treatment, observed that it worked, and have now spent decades trying to understand how it works. Understanding how DBS works is important, as it will allow not only for the optimization of the technique to treat Parkinson’s, but also for the use of the technology in the treatment of other neurological and psychiatric disorders. The longest standing hypothesis for how DBS works is called the ‘classic rate model.’ This hypothesis argues that the problem with the loss of dopamine in the basal ganglia is the that neurons in the basal ganglia become overactive, and this leads to Parkinson’s symptoms. The stimulation, this model argues, somehow dampens activity in the basal ganglia and relieves symptoms, which is why DBS’s effects are similar to basal ganglia lesions2. Recent work, however, suggests that it is not that simple. In fact, studies have found that DBS actually increases overall firing of basal ganglia neurons2. What is clear is that the firing patterns of basal ganglia neurons are altered by stimulation, and that the altering of their firing is therapeutic. For example, another argument is that in Parkinson’s, neurons in the basal ganglia fire in a bursting pattern, with synchronous highs and lows in activity which leads to Parkinson’s symptoms2. DBS, according to this view, delivers relatively constant stimulation which prevents this bursting activity.
New theories are also emerging supporting a neuroprotective role for DBS. This is especially exciting as the ultimate goal in treating neurodegenerative disease is the slowing or halting of disease progression, rather than just treating symptoms. One study found that in a model of Parkinson’s in monkeys, DBS resulted in significantly less dopamine neuron loss3. It’s possible that the electrical stimulation is somehow increasing the production of neuroprotective proteins that slow the degeneration of dopamine neurons4. Thus, while we still don’t know exactly how DBS works, our ability to precisely control both the location of the electrodes with surgical advancements and the type of stimulation used has led to new uses for DBS, particularly in the treatment of psychiatric disorders.
New uses for DBS
The Food and Drug Administration approved the use of DBS as a treatment for Parkinson’s Disease in 19972. Since then, it has been approved to treat obsessive compulsive disorder (OCD) and epilepsy, and is undergoing clinical trials as a potential treatment for chronic pain and major depression1. Interestingly, it is believed that DBS works differently when used to treat psychiatric conditions such as OCD. When surgeons target regions in the basal ganglia with leads to treat Parkinson’s, they aim for grey matter, or nodes in the brain that contain a group of neuron cell bodies. On the contrary, DBS in the treatment of OCD targets white matter tracts, or bundles of axons sending information from one region to another2. Stimulation, in this case, is believed to affect networks of brain regions, perhaps changing the activity patterns of several regions at once.
What Are the Limitations?
As with any treatment in which the underlying mechanism of action is not well understood, it is important to consider the limitations of DBS. There are serious risks associated with brain surgery, and many individuals do not meet the criteria necessary to qualify for DBS. Additionally, while the ability of the brain to adapt is one of its great strengths, it also means that the brain can adapt to stimulation. In the case of OCD, one study found that when stimulation was turned off in DBS patients, their symptoms were worse than they had been before they received the implant5. Therefore, it is critical to continue to study how DBS works in order to make it an even more effective treatment for a wide variety of neurological and psychiatric disorders.
References:
- Shukla, A. W. & Okun, M.S. Surgical Treatments of Parkinson’s Disease: Patients, Targets, Devices, and Approaches. Neurotherapeutics 11, 47-59 (2014).
- Ashkan, K., Rogers, P., Bergmann, H., Ughratdar, I. Insights into the Mechanisms of Deep Brain Stimulation. Nature Reviews Neurology 13, 548-554 (2017).
- Wallace, B. A. et al. Survival of midbrain dopaminergic cells after lesion or deep brain stimulation of the subthalamic nucleus in MPTP-treated monkeys. Brain130, 2129–2145 (2007).
- Ho, D. X., Tan, Y. C., Tan, J., Too, H. P. & Ng, W. H. High-frequency stimulation of the globus pallidus interna nucleus modulates GFRα1 gene expression in the basal ganglia. Clin. Neurosci.21, 657–660 (2014).
- Ooms, P. et al. Rebound of Affective Symptoms Following Acute Cessation of Deep Brain Stimulation in Obsessive-compulsive Disorder. Brain Stimulation 7, 727-731 (2014).
Image References:
Cover image from Wikimedia Commons: Andreashorn, Creative Commons Attribution-Share Alike 4.0 International https://commons.wikimedia.org/wiki/File:Deep_brain_stimulation_electrode_placement_reconstruction.png
Figure 1 from Wikimedia Commons: Was a Bee, Creative Commons Attribution 3.0 Unported https://commons.wikimedia.org/wiki/File:Typical_deep_brain_stimulation_setup.jpg

{kind=link}
{kind=link}