
October 30, 2018
Written by: Katerina Placek
Repetitive behaviors. Inability to comprehend common grammatical structure. Muscle spasms. Profound apathy. Not understanding what the words “can opener” refer to. What could all of these seemingly unrelated problems possibly have in common? They are all symptoms of a fatal neurodegenerative disease called frontotemporal degeneration, or FTD, that affects adults as early as age 40. Even though an estimated 50-60,000 Americans suffer from FTD,1 individuals with these symptoms are often misdiagnosed with Alzheimer’s disease. Read on to learn about how neuroscientists have begun to unravel the complexities of this lesser known form of dementia.
In 1892, Czech neurologist and psychiatrist Arnold Pick recorded the first known incidence of FTD: an adult patient with progressive loss of ability to understand or produce speech and behavioral disturbances.2 According to accepted practice of nomenclature at the time, he referred to his patient’s condition as ‘Pick disease.’ By examining the structure of this and similarly-affected patients’ brains post mortem, Pick determined that the cause of these symptoms were focal areas of degeneration in the outer layers of the frontal and temporal lobes of the brain (see Figure 1). Interestingly, patients with Pick disease did not have memory loss and, when German neuropathologist Alois Alzheimer examined their brain tissue under the microscope in 1901, he observed abnormal proteins different from those he observed in patients with Alzheimer’s disease and called them ‘Pick bodies’ to mark their distinction.

Although Pick and Alzheimer distinguished FTD from Alzheimer’s disease almost a century ago, individuals with FTD are still often misdiagnosed as having Alzheimer’s disease. This isn’t surprising, given that Alzheimer’s disease is the most common cause of dementia. However, FTD and Alzheimer’s disease are distinct in key ways:
First, FTD affects individuals earlier in life. Alzheimer’s disease typically affects individuals after age 65, whereas FTD affects individuals in their 40s-60s. Thus, while Alzheimer’s disease is the most common cause of dementia, FTD is the most common cause of early-onset dementia. Because it affects individuals still in the workforce, FTD carries twice the economic burden of Alzheimer’s disease.3
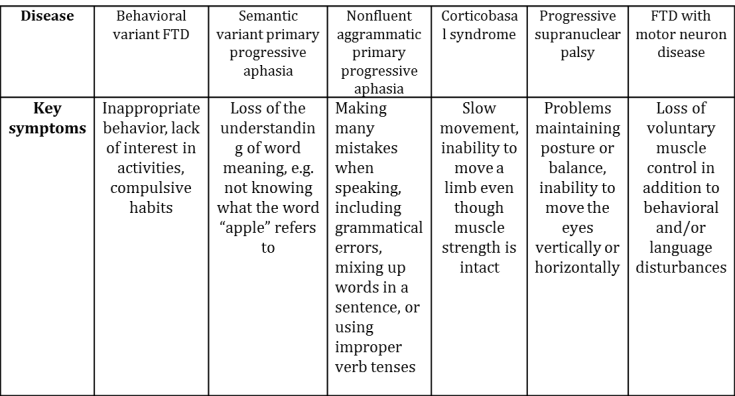
Second, as Pick observed, patients with FTD don’t have the same symptoms as patients with Alzheimer’s disease – instead of progressive memory loss, they experience profound behavior and personality change, loss of language, and/or impaired movement. We now know that there are six – yes six – different forms that FTD can take (see Table 1), each of which features symptoms distinct from the hallmark degradation of short, then longer-term memories in Alzheimer’s disease.
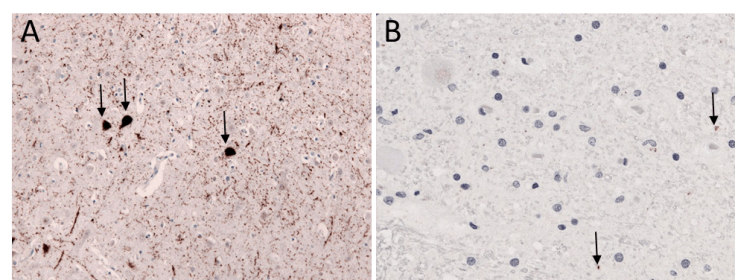
Third, as both Pick and Alzheimer noted, FTD affects the brain differently than Alzheimer’s disease. As discussed in a previous pennneuroknow post , a diagnosis of Alzheimer’s disease requires the presence of key misfolded proteins called amyloid beta plaques and neurofibrillary tangles. However, FTD can feature one of two different types of misfolded protein: tau (Figure 3A) or TAR DNA-binding protein 43 kD (TDP-43, for short; Figure 3B).4 The Pick bodies that Alzheimer identified in 1901 are actually misfolded tau proteins, although scientists still refer to them as Pick bodies to this day!
So why does the distinction of FTD from Alzheimer’s disease matter? Both diseases are fatal, with survival from symptom onset ranging 2-10 years, and no known cure for either disease exists. However, understanding the differences between these forms of dementia is a necessary first step in understanding the causes of disease – and developing specialized treatments for each cause. While FTD is a startlingly complex disease – taking six different forms, and associated with two different misfolded proteins – the knowledge gained from neuroscientists over the past century is bringing the prospect of a targeted cure within reach.
References:
- Knopman, D. S. & Roberts, R. O. Estimating the number of persons with frontotemporal lobar degeneration in the US population. J Mol Neurosci 45, 330–335 (2011).
- Kertesz, A. & Kalvach, P. Arnold Pick and German Neuropsychiatry in Prague. Arch Neurol 53, 935–938 (1996).
- Galvin, J. E., Howard, D. H., Denny, S. S., Dickinson, S. & Tatton, N. The social and economic burden of frontotemporal degeneration. Neurology 10.1212/WNL.0000000000004614–9 (2017). doi:10.1212/WNL.0000000000004614
- Irwin, D. J. et al. Frontotemporal lobar degeneration: defining phenotypic diversity through personalized medicine. Acta Neuropathol 129, 469–491 (2014).
Image References:
Cover Image: Photo by Evan Dennis on Unsplash
Figure 1: Image adapted from Wikimedia Commons; CC BY-SA 3.0. https://commons.wikimedia.org/wiki/File:Frontotemporal_degeneration.jpg
Figure 2A: Image adapted from Wikimedia Commons, CC BY-SA 3.0. https://commons.wikimedia.org/wiki/File:FTDP-17_TAU_cortex.jpg
Figure 2B. Image adapted from Wikimedia Commons; CC BY-SA 4.0. https://commons.wikimedia.org/wiki/File:ALS-TDP-43_IHC.jpg

{kind=link}
{kind=link}
Leave a comment