
April 4th, 2023
Written by: Lisa Wooldridge
Imagine you’re watching a puppy or a kitten sleep (or check out this video). For many minutes, they’re totally still. Then out of nowhere, their paws start twitching vigorously. Yet they stay peacefully asleep. It’s an uncanny glimpse into a most perplexing brain state – REM sleep.
What is REM sleep?
Contrary to popular belief, your brain never stops working, even when you’re asleep. Throughout a good night’s sleep, you’ll cycle through several sleep types, each with different varieties and intensities of brain activity. REM sleep, or Rapid Eye Movement sleep, is the last type of sleep you experience during each cycle, and the last you’ll typically experience before you wake up in the morning. Surprisingly, when you reach REM sleep, your brain becomes very active again- similar to a wakeful state – even though you’re sound asleep. In fact, it’s quite hard to wake someone up from this final sleep stage1. This wake-like brain activity is probably why REM sleep is associated with vivid dreams.1 The major difference between REM sleep and wake involves not your brain, then, but your body. During REM sleep, your brain puts the brakes on nearly all of your muscle movements, a phenomenon called REM muscle atonia. The exceptions are the muscles for breathing, and the muscles that control our eyes – that’s how we get the “rapid eye movements” from which REM sleep takes its name.
The brain-body brake pedal
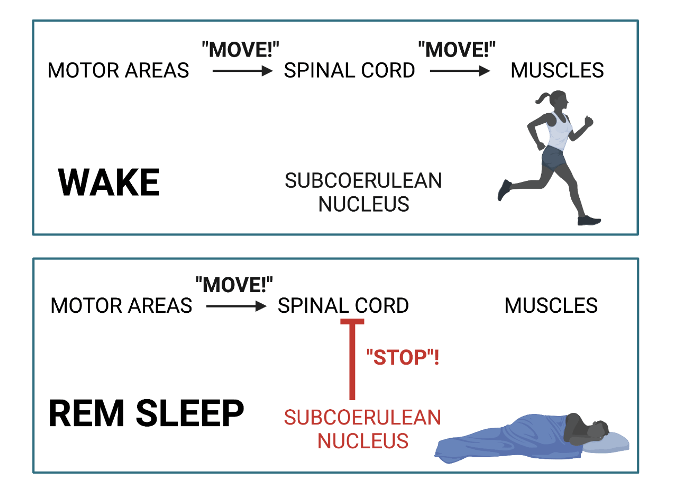
REM muscle atonia is most likely due to the activity of a part of the brain called the subcoerulean nucleus. This neural center, stationed deep in the base of your brain, is quiet the majority of the time, but becomes very active during REM sleep1. In its active state, it acts as the neural brake pedal, prompting a flood of “stop!” messages in the spinal cord. While you’re awake, the spinal cord receives signals from motor control areas in the brain and disseminates them to motor neurons in the rest of your body, telling your muscles to move (Figure 1, top panel). During REM sleep, these motor region signals still come down – but when they reach the spinal cord, they’re overwhelmed by those “stop!” messages from the subcoerulean nucleus, and your muscles never get the message (Figure 1, bottom panel).
When the brakes fail
The muscle-braking system is not foolproof. Sometimes, the brake gets stuck on as you wake up. This results in the somewhat frightening experience of sleep paralysis – where you wake up still unable to move and, sometimes, with the terrifying feeling that your nightmares are still happening. And occasionally, a strong signal will get through the messages from the subcoerulean nucleus – resulting in the muscle twitches you watched earlier. Sleep paralysis can be scary but is generally harmless; twitches, too, are harmless. But what happens when the brake pedal fails entirely?
Damage to or poor regulation of the subcoerulean nucleus often prevents REM muscle atonia, and causes REM Sleep Behavior Disorder. Though they remain sound asleep, patients with REM Sleep Behavior Disorder (RBD for short) move around during REM sleep, often injuring themselves and their bedmates. These movements range from frequent twitching to shouting or laughing, to fully acting out their dreams – sometimes violently. Without the alertness that accompanies wakefulness, acting out dreams can seriously injure RBD patients or their bedmates.2
RBD is common in patients with other sleep disorders, especially narcolepsy.3 Many additional cases start after patients begin antidepressant medications that interfere with serotonin.4 Strokes, tumors, or damage that impact the subcoerulean nucleus have also resulted in RBD. Sadly, in about 65% of cases with no other obvious cause, RBD appears to be an early sign of neurodegeneration.1 More specifically, neurodegenerative diseases such as Parkinson’s that are associated with accumulations of a protein called alpha-synuclein are often preceded by years or even decades by RBD. In fact, accumulation of these proteins in the subcoerulean nucleus in mice is enough to produce RBD and, a few months later, motor disorders that resemble Parkinson’s.5,6 This strongly suggests that the same processes that cause Parkinson’s Disease can cause RBD when they originate in the subcoerulean nucleus.
While treating RBD doesn’t stop neurodegeneration in these patients, the RBD itself is relatively easy to manage. This can be achieved by treating the underlying conditions or with a number of different prescription and over-the-counter medications. For example, narcolepsy patients tend to see improvements with medications that interact with the neurotransmitter orexin; for patients whose symptoms were brought on by antidepressants, switching to a different type usually eases them. For many other cases, melatonin seems to do the trick! It’s unclear why, but high doses of the common over-the-counter sleep aid promotes REM muscle atonia, and taking it nightly before bed is often enough to restore the brakes and get RBD patients back to dreaming peacefully.7
References
- Peever J, Fuller PM. The Biology of REM Sleep. Curr Biol. 2017 Nov 20;27(22):R1237-R1248.
- McCarter SJ, St Louis EK, Boswell CL, Dueffert LG, Slocumb N, Boeve BF, Silber MH, Olson EJ, Morgenthaler TI, Tippmann-Peikert M. Factors associated with injury in REM sleep behavior disorder. Sleep Med. 2014 Nov;15(11):1332-8. Nightingale S, Orgill JC, Ebrahim IO, de Lacy SF, Agrawal S, Williams AJ. The association between narcolepsy and REM behavior disorder (RBD). Sleep Med. 2005 May;6(3):253-8.
- Winkelman JW, James L. Serotonergic antidepressants are associated with REM sleep without atonia. Sleep. 2004 Mar 15;27(2):317-21.
- Shen Y, Yu WB, Shen B, Dong H, Zhao J, Tang YL, Fan Y, Yang YF, Sun YM, Luo SS, Chen C, Liu FT, Wu JJ, Xiao BG, Yu H, Koprich JB, Huang ZL, Wang J. Propagated α-synucleinopathy recapitulates REM sleep behaviour disorder followed by parkinsonian phenotypes in mice. Brain. 2020 Dec 5;143(11):3374-3392.
- McGrane IR, Leung JG, St Louis EK, Boeve BF. Melatonin therapy for REM sleep behavior disorder: a critical review of evidence. Sleep Med. 2015 Jan;16(1):19-26.
Cover Photo by DANNY G on Unsplash
Figure 1 created by Lisa Wooldridge using Biorender.com
