
June 2, 2020
Written by: Sarah Reitz
Aphasia is a language disorder affecting at least 2 million Americans that impairs the ability to produce or comprehend speech, along with the ability to read or write1. It can result from any injury or disease that damages the language centers of the brain2, including autoimmune encephalitis (AE). To better understand aphasia in the context of AE, it is important to first know how the brain processes language as well as the different types of aphasia that can occur as a result of damage to any of these language centers.
How is language processed in the brain?
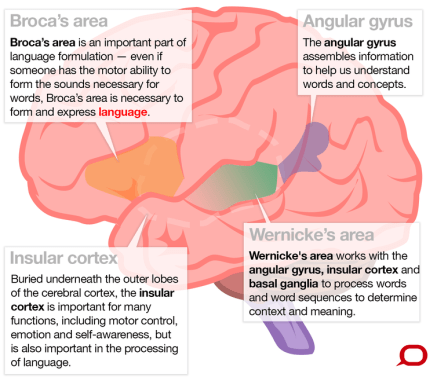
The ability to comprehend and use language is a complicated process that involves many regions of the brain. A few of the areas typically associated with language include Broca’s area, Wernicke’s area, the insular cortex, and the angular gyrus (Figure 1). Broca’s area, found in the left frontal cortex, together with the insular cortex, are important for producing language (called expressive language).
Wernicke’s area and the angular gyrus, both located in the temporal lobe, play a major role in understanding the context and meaning of language (called receptive language)3-5.
What is aphasia?
There are many different types of aphasia, ranging from mild forms that involve occasionally struggling to find the right words, to much more severe forms that limit nearly all forms of communication. The level of aphasia varies dramatically from patient to patient, with each person having his or her own unique language difficulties. Still, aphasia has been classified into a few main subtypes based on the main language deficits experienced by the patient (Figure 2).
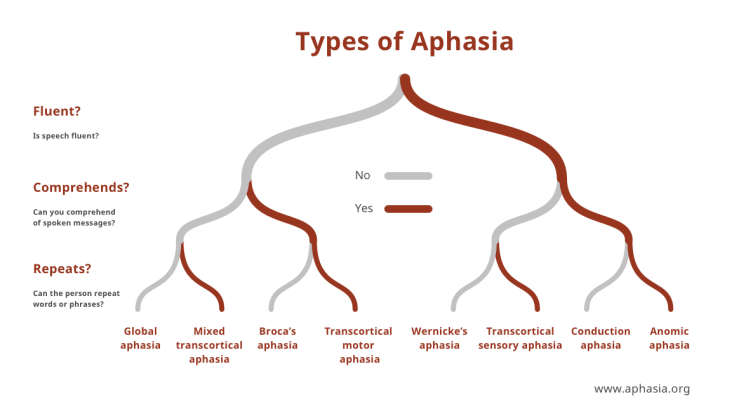
One of the more mild forms of aphasia is anomic aphasia. People with anomic aphasia have difficulty finding the right words or naming things, sometimes describing the phenomenon as having the word on the tip of their tongue. However, they can often describe the word in detail, such as “the blue pants made of denim” when they are looking for the word “jeans”. Sometimes, patients will only have difficulty naming specific categories of words (such as nouns, or only words related to a specific activity), though the reasons for this are unknown. They are able to speak and write fluently, though they will often use vague terms to describe the word they are having difficulty with. Additionally, the ability to read remains intact6.
Intermediate forms of aphasia include Broca’s aphasia and Wernicke’s aphasia2,6. Like their names suggest, these types of aphasia result mainly from damage to either Broca’s or Wernicke’s areas. Broca’s aphasia is sometimes known as “non-fluent aphasia” due to the extreme difficulties in speech production experienced by the patient. Expressive language is severely limited, with speech oftentimes consisting of fewer than 4 words at a time. In contrast, patients with Wernicke’s aphasia can still produce fluent speech without much effort, but their ability to understand the meaning of words is impaired. So, while they can connect words into sentences and speak easily, the sentences themselves will usually not make sense and often consist of jumbled, disjointed words. Because comprehending the meaning of words is damaged, patients with Wernicke’s aphasia also have a very difficult time with reading and writing. Other people experience various combinations of these two types of aphasia, which are classified in Figure 2 based on the symptoms exhibited6.
The most severe form of aphasia is global aphasia. This disorder severely limits both receptive and expressive language. The ability to read and write is nearly nonexistent, as patients can neither comprehend nor produce language. While their language abilities are almost absent, patients with global aphasia can have normal non-language related intellectual and cognitive capabilities2,6.
Interestingly, aphasia is not limited to written and spoken languages. Because visual languages like sign language are also processed and produced by the language centers of the brain7, they can also be impaired, causing sign language speakers to lose the ability to use or understand sign language2,8.
Aphasia in autoimmune encephalitis
Aphasia is caused by damage to the language centers of the brain. While strokes are the most common cause9, any disease or injury that damages the regions of the brain involved in language can cause aphasia. These include things like brain tumors, traumatic brain injuries, progressive neurodegenerative disorders, and autoimmune encephalitis. The specific regions damaged by the injury or disease will determine which type of aphasia results2.
There are multiple case reports that document instances of aphasia in patients with autoimmune encephalitis. Many of these patients suffer specifically from anti-NMDAR encephalitis10-13, although aphasia has also been recorded in other types of AE14. A 5-year study of 501 patients diagnosed with anti-NMDAR encephalitis tracked symptom development and found that speech problems are common early symptoms. Around 70% of patients over the age of 12 showed some form of a speech disorder, while nearly 85% of those younger than 12 exhibited symptoms of a speech disorder10! In at least one case, however, aphasia developed 19 months after the first AE symptoms, suggesting that there is no definitive timeframe for development of this disorder12.
Various types of aphasia have been reported with AE. Some patients show symptoms similar to Broca’s aphasia, with effortful speech and trouble producing language11. Others have reported more severe, global aphasia consisting of trouble both comprehending and expressing language12. In one case, a woman with anti-NMDAR encephalitis had persistent aphasia for 6 months with no other symptoms typically experienced in AE13. What is clear is that aphasia in AE, just like aphasia caused by other injuries or disease, exists on a spectrum and can include any number of language impairments.
Recovery from aphasia
Because so many injuries and diseases can cause aphasia, there is no standard treatment for the disorder. Each patient must be treated individually, taking many factors into consideration. However, speech-language therapy is critical for all types of aphasia2.
One major factor considered in treatment plans is the cause of the aphasia. Aphasias resulting from neurodegenerative disorders show much lower rates of recovery due to the progressive nature of the neurodegeneration15. However, aphasia resulting from other causes will usually show at least some degree of improvement with proper treatment2. In the case of autoimmune encephalitis, aphasia symptoms tend to disappear once appropriate treatment for the underlying encephalitis is administered11-14.
Other factors that may determine a patient’s outcome are the type of aphasia the patient is experiencing as well as the level of communication skills prior to aphasia onset. A rich vocabulary before the onset of aphasia tends to predict a better recovery2.
Advancements in aphasia research, and the underlying diseases that cause it will continue to inform better treatments, improving outcomes for millions of people across the world and helping them regain their communication abilities.
Image References:
Cover image via Pxfuel, https://www.pxfuel.com/en/free-photo-xpnmp
Figure 1 image via The Conversation, CC BY-ND. https://theconversation.com/what-brain-regions-control-our-language-and-how-do-we-know-this-63318
Figure 2 image via the National Aphasia Association, https://www.aphasia.org/graphic-assets/
References:
- Aphasia Statistics. National Aphasia Association Available at: https://www.aphasia.org/aphasia-resources/aphasia-statistics/. (Accessed: 2nd May 2020)
- Damasio AR (1992) Aphasia. NEJM 326(8):531-539
- Friederici AD (2011) The brain basis of language processing: from structure to function. Physio Review. 91(4)1357-1392
- Van Ettinger-Veenstra H, McAllister A, Lundberg P, Karlsson T, Engstrom M (2016) Higher language ability is related to angular gyrus activation increase during semantic processing, independent of sentence incongruency. Hum. Neurosci. 10:110
- Oh A, Duerden EG, Pang EW (2014) The role of the insula in speech and language processing. Brain Lang. 135:96-103
- Aphasia Definitions. National Aphasia Association Available at: https://www.aphasia.org/aphasia-definitions/. (Accessed: 2nd May 2020)
- Hickok G, Love-Geffen T, Klima ES (2002) Role of the left hemisphere in sign language comprehension. Brain and Lang 82:167-178
- Damasio A, Bellugi U, Damasio H, Poizner H, Van Gilder J (1986) Sign language aphasia during left-hemisphere amytal injection. Nature 322:363-365
- Aphasia FAQs. National Aphasia Association. Available at: hyyps://www.aphasia.org/aphasia-faqs/. (Accessed: 2nd May 2020)
- Titulaer M et al. (2013) Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study. Lancet Neurol 12:157-165
- Bhat P, Ahmed A, Jolepalem P, Sittambalam C (2018) A case report: anti-NMDA receptor encephalitis. Journal of Comm Hospital Internal Med Perspect 8(3):158-160
- Mario LSJ, Ramiro R, Ruth DVA, Jose F, Carmen OL, Mariana EN (2017) Cortical aphasia and apraxia as main clinical presentation of anti-NMDAR encephalitis relapse with a positive CSF PCR for cytomegalovirus. Neuropsych 7(5):620-628
- Constantinides VC et al (2018) Anti-NMDA receptor encephalitis presenting as isolated aphasia in an adult. Neurocase 24(4)188-194
- Hayata Y, Hamada K, Sakurai Y, Sugimoto I, Mannen T, Takahashi Y (2014) Anti-glutamate ε2 receptor antibody-positive and anti-N-methyl-D-aspartate receptor antibody-negative lobar encephalitis presenting as global aphasia and swallowing apraxia. Case Rep Neurol 6:291-296
- Primary Progressive Aphasia. National Aphasia Association Available at: https://www.aphasia.org/aphasia-resources/primary-progressive-aphasia/. (Accessed 12th May 2020)

Leave a comment