
April 14, 2020
Written by: Sarah Reitz
Anyone reading the news lately has likely seen the term “anosmia” in coverage of the novel coronavirus. Anosmia, a partial or complete loss of smell, appears to be one of the early symptoms of COVID-19, and may even be present in otherwise asymptomatic carriers of the disease. In fact, data from the COVID Symptom Tracker app from March 24-29, 2020 showed that 59% of COVID-19 positive patients reported a loss of smell and taste, making it an even stronger predictor of a positive diagnosis than fever1. Fortunately, sense of smell appears to return to normal upon recovery from the disease. With anosmia in the cultural conscious more than ever before, let’s dive into the science behind losing this important sense.
The Olfactory System
Before understanding anosmia, we first have to understand how the brain actually processes and perceives smells. We perceive odors when chemical compounds in the air, called odorants, enter the nose. When these odorants reach the nasal epithelium, a membrane on the inside of the nose, they bind to and activate receptors on olfactory neurons, causing them to fire off a message to the brain (Figure 1).
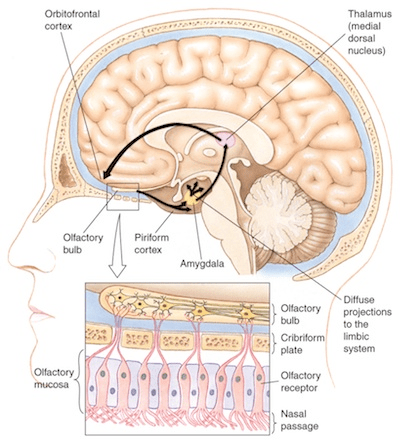
There are hundreds of different olfactory receptors, clustered into groups called glomeruli that are each activated by distinct sets of odorants. The message from the olfactory neurons travels to other neurons in the olfactory bulb, a region at the front of the brain that processes smell. From here, signals are sent to many areas of the brain, including the olfactory cortex, the hippocampus, the orbitofrontal cortex, and the amygdala.
Diagnosing Anosmia
Over the years, a set of standardized smell tests has been developed to help identify impairments to this sense. The most commonly used test, developed here at the University of Pennsylvania, is called the University of Pennsylvania Smell Identification Test, or UPSIT2. It consists of 40 scratch & sniff odors that the patient must identify from a given list of choices. The number of incorrect answers, as well as which types of smells were misidentified, is then used to determine the extent of smell loss. Sometimes, patients will be asked to first take the shorter version of this test (B-sit, or Brief Smell Identification Test), as it contains only 12 odors. If the results are abnormal they will then take the full UPSIT for a more complete examination of their anosmia.
Causes of Anosmia
While lately anosmia always seems to be mentioned in the same breath as COVID-19, a number of injuries or diseases can actually damage a person’s sense of smell. About 20% of cases occur after head injuries, which can damage the olfactory system at various points2. For example, some injuries may damage the nose and olfactory nerves themselves, while others (such as concussion) may damage brain regions involved in perceiving smell. Often, this type of damage can be diagnosed by imaging the brain using MRI3.
Aside from traumatic head injuries, neurodegenerative diseases — specifically Alzheimer’s disease (AD) and Parkinson’s disease (PD) — have also been linked to a diminished sense of smell. One study found that over 90% of patients with either AD or PD have some level of smell impairments4. In AD, the patient’s sense of smell declines steadily over time. Researchers believe the same proteins responsible for the memory impairments that occur in AD are also responsible for the reduced ability to smell. In fact, high levels of these proteins — β-amyloid and tau — have been found in many brain regions involved in olfaction, including the entorhinal and piriform cortex, the olfactory bulb, and anterior olfactory nucleus5.
While loss of smell is a gradual process in patients with AD, a diminishing sense of smell occurs much more rapidly in PD, reaching its peak early in the course of the disease2. Some studies even suggest that smell impairments may occur years before the classical movement symptoms of PD, making it a potential predictor of who is at risk of developing the disease. Similar to AD, researchers suspect that loss of smell in PD may be due to increased levels of misfolded proteins, in this case alpha-synuclein, in olfactory brain regions. This idea is supported by a study that examined the olfactory bulbs of PD patients who had died. The researchers found that patients with higher levels of alpha-synuclein in the olfactory bulb also had lower total volume of glomeruli, which would explain the impaired sense of smell6,7.
A much less common form of anosmia is congenital anosmia, a condition where patients are seemingly born with no ability to smell. While congenital anosmia usually occurs randomly, there are some cases where it is passed down through families. Interestingly, congenital anosmia appears to be caused by mutations in a number of different genes. One gene responsible for the anosmia in some of these families is a gene called CNGA2, which codes for a subunit of an olfactory channel8. As mentioned earlier, these olfactory channels are what become activated by odorants, ultimately triggering olfactory neurons to send a message to the brain where the smell is perceived. Mutations in other genes that result in congenital anosmia are still being discovered, however.
Finally, a number of bacterial and viral infections can also cause anosmia. While we don’t know for sure, researchers believe that viruses or bacteria entering the body through the nose infect the olfactory nerves, ultimately killing some of the neurons9. Depending on how many neurons are lost, various degrees of smell loss can occur. Luckily, olfactory neurons are one of the few types of neurons that constantly regenerate throughout our lives, meaning that anosmia caused by infection usually returns to normal a few weeks after infection.
Recovery From Anosmia
Regaining a fully functional sense of smell greatly depends on the underlying cause of the anosmia. For example, anosmia caused by genetic mutations or neurodegenerative diseases is unlikely to improve. On the other hand, anosmia resulting from viral or bacterial infections usually returns to normal a few weeks after the infection is cleared, due to the regeneration of olfactory neurons mentioned earlier10.
Recovery from anosmia caused by traumatic head injury is much harder to predict, however. There are many factors that affect recovery from this type of anosmia, but the two that seem to be most linked to degree of recovery are the extent of smell loss and the age when the injury occurred. Patients with mild or moderate loss of smell, called hyposmia, are twice as likely to improve compared to those with total smell loss. Additionally, younger patients are more likely to improve compared to older patients. Specifically, one study found that recovery dropped drastically after age 74, though the exact reasons are not fully understood2. Interestingly, the cause of the initial head injury does not appear to predict how well the sense of smell will recover.
Living With Anosmia
For those who do not recover their full sense of smell, adjusting to a life with hyposmia or anosmia can be a challenge. Smell loss impairs both smell and taste, as tasting heavily relies on odors from food (hence why some people may plug their nose when eating something unpleasant). The basic tastes (sweet, sour, bitter, salt, and umami) as well as ability to sense spice is still intact however, so many patients learn to adjust their cooking to emphasize these flavors.
While our sense of smell allows us to enjoy the world around us, it also protects us. Without the ability to smell things like smoke, natural gas, or spoiled food, people with anosmia are at an increased risk of injury or even death from these causes11. Hopefully, as researchers learn more about these conditions, they will be able to improve outcomes for patients with anosmia, and help those who don’t recover to better adjust to their new normal.
Image References:
Cover image by Dennis Wong via Flickr, https://www.flickr.com/photos/denniswong/3309276218
Figure 1 by Aintavatu via https://brain-for-ai.fandom.com/wiki/Olfactory_pathway CC-BY-SA
References:
- Neuroscience News (2020) Loss Of Smell And Taste Is Strongest Predictor Of Early COVID-19 Infection – Neuroscience News. [online] Available at: <https://neurosciencenews.com/covid-19-smell-taste-16056/> [Accessed 12 April 2020].
- Devere R (2012) Smell and taste in clinical neurology: Five new things. Neurol Clin Pract 2(3):208-214. doi: 10.1212/CPJ.0b013e31826af199
- Doty RL, Yousem DM, Pham LT, Kreshak AA, Geckle R, Lee WW (1997) Olfactory dysfunction in patients with head trauma. Arch Neurol 54(9):1131-1140
- Devanand DP et al (2000) Olfactory deficits in patients with mild cognitive impairment predict Alzheimer’s disease at follow-up. Am J Psychiatry. 157(9):1399-1405.
- Devere R (2009) Olfactory testing in the diagnosis of Alzheimers disease and other neurodegenerative disorders. Pract Neurol. 34–41.
- Haehner A, Hummel T, Reichmann H (2014) A clinical approach towards smell loss in Parkinson’s disease. J Parkinsons Dis. 4(2):189-195
- Zapiec B et al (2017) A ventral glomerular deficit in Parkinson’s disease revealed by whole olfactory bulb reconstruction. Brain 140(10):2722-2736
- Reza Sailani M et al (2017) Isolated congenital anosmia and CNGA2 mutation. Sci Rep. 7:2667
- Bohmwald K, Galvez N, Rios M, Kalergis AM (2018) Neurologic alterations due to respiratory virus infections. Front Cell Neurosci. Doi: 10.3389/fncel.2018.00386
- London B et al (2008) Predictors of prognosis in patients with olfactory disturbance. Ann Neurol 63(2):159-166
- Miwa T et al (2001) Impact of olfactory impairment on quality of life and disability. Arch Otolaryngol Head Neck Surg 127(5):497-503
