
September 15, 2020
Written by: Rebecca Somach
“Sit still! Pay attention! What is wrong with you?”
It would be out of line for adults to say these kinds of things to each other, but most people can think back to a time in school or at home when they were admonished just like this for moving around, daydreaming, or not focusing. This type of language is meant to teach children respect and patience. However, there are a subset of children that appear to be disrespectful and rude because they refuse to sit still no matter how often they are yelled at. Forgetfulness, distraction, lack of organization and not paying attention to direct comments are all signs of Attention-Deficit/Hyperactivity Disorder (ADHD). It is most often diagnosed in children and as of 2016, the Center for Disease Control reported that 6.1 million children had ADHD1. While most cases are diagnosed in children, the disorder does not necessarily go away after childhood. Worldwide, some studies have estimated that 2.8% of adults may have ADHD2, including those diagnosed as children and adults. ADHD has social and psychological factors, but it is ultimately caused by changes that occur in the brain.
You might think that with a disorder called “hyperactivity disorder,” lots of areas of the brain would be, well, hyperactive. However, it is not quite that simple. In fact, some of the treatments for ADHD include stimulants3, which seems counterintuitive. Why stimulate a hyper brain? ADHD is a disorder which is partially caused by an imbalance of neurotransmitters. One of these is norepinephrine4 which is associated with attentiveness and alertness. Another neurotransmitter involved is dopamine5 which is often associated with happiness and pleasure, but is also important for learning and attention.
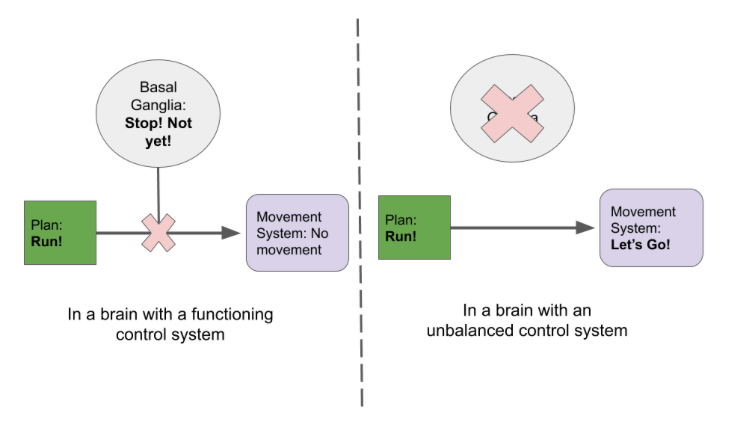
It is important to know what neurotransmitters are unbalanced in ADHD, but it is also important to know where they are unbalanced. In some regions of the brain, a lack of neurotransmitter can actually lead to more movement or activity. Some regions of the brain are meant to suppress impulses, including the prefrontal cortex and the basal ganglia. Suppressing impulses is an important survival trait for many animals. When hunting, if an animal isn’t able to pounce at the right time, they might miss out on dinner. Even worse, if an animal moves when they aren’t supposed to, they might become dinner! These brain regions help suppress movement until the rest of the brain determines that it is the right moment to act (see Figure 1). If the neurons in these regions are not being sufficiently activated by norepinephrine and dopamine, they can’t inhibit other parts of the brain. That lack of inhibition ultimately leads to impulsive behavior.
Stimulants activate these areas of the brain involved in inhibition to reduce impulsive behavior. Examples of this can include Adderall. Stimulants boost the overall levels of neurotransmitters in the brain or are substances that are similar to the natural transmitter6. Some drugs for ADHD aren’t technically stimulants, such as Atomoxetine7. Atomoxetine keeps the neurotransmitters near the receptors for a longer period of time. That means that the body will still produce the same amount of neurotransmitter but there are more chances for it to act on the neurons. Both of these drugs ultimately lead to more signaling in the regions of the brain that have an imbalance in neurotransmitters (see Figure 2). Some patients may need one type of drug and not another. Since much is known about the ways neurotransmitters work in these regions of the brain, there are different options available to patients.

Other changes may occur in the brain of someone with ADHD beyond the neurotransmitter level. Some studies have found that the physical structure of the brain is different in people with ADHD. Several studies have found that the gray matter, or the brain tissue composed of the cell bodies of the neurons, is thinner in people that had been diagnosed with ADHD in childhood compared with control subjects8 and that the overall volume of the brain is reduced9. One study followed the development of the thickness of the cortex in subjects with ADHD and found that it developed slower than in subjects without ADHD10. While drugs that replace and supplement neurotransmitters can be extremely helpful, they may not help with these structural changes that appear to be impaired throughout development.
To complicate ADHD a little further, there is also a symptom known as ‘hyperfocus’ 11 which presents as the complete opposite of what one would expect of ADHD. In this state, a person will focus on one thing completely, sometimes for hours at a time. As we learn more about ADHD, it is becoming increasingly clear that it is actually a disorder in directing attention, not of a lack of attention entirely. ADHD does not present the same way in every individual. Some will hyperfocus, others will not. Some will be constantly distracted and overly excited, while others will have a lack of organization instead. As our society becomes more aware of mental health disorders, it is also worth realizing that some disorders are not as obvious as we might believe. As we interact with more children and adults with ADHD it is important to recognize that they are not defined by their disorder. They are not necessarily trying to cause disrespect by not sitting still at school or in a meeting. They are confronting a challenge that might be caused by changes in neurotransmitters, not their desire to distract a whole room. Just like we wouldn’t tell someone in a leg cast they are weak because they can’t stand up, we also wouldn’t tell a student with ADHD that they are bad because they have trouble staying in their chair. Both are disorders with treatment options, neither are a reason to judge someone.
Cover image: Pixabay. User KokomoCole
Figures 1 and 2 created with Google Slides
References:
1. CDC. Data and Statistics About ADHD | CDC. Centers for Disease Control and Prevention https://www.cdc.gov/ncbddd/adhd/data.html (2020).
2. Fayyad, J. et al. The descriptive epidemiology of DSM-IV Adult ADHD in the World Health Organization World Mental Health Surveys. Atten. Deficit Hyperact. Disord. 9, 47–65 (2017).
3. Magnus, W., Nazir, S., Anilkumar, A. C. & Shaban, K. Attention Deficit Hyperactivity Disorder (ADHD). in StatPearls (StatPearls Publishing, 2020).
4. Biederman, J. & Spencer, T. Attention-deficit/hyperactivity disorder (adhd) as a noradrenergic disorder. Biol. Psychiatry 46, 1234–1242 (1999).
5. Madras, B. K., Miller, G. M. & Fischman, A. J. The Dopamine Transporter and Attention-Deficit/Hyperactivity Disorder. Biol. Psychiatry 57, 1397–1409 (2005).
6. Calipari, E. S. & Ferris, M. J. Amphetamine Mechanisms and Actions at the Dopamine Terminal Revisited. J. Neurosci. 33, 8923–8925 (2013).
7. Garnock-Jones, K. P. & Keating, G. M. Atomoxetine: a review of its use in attention-deficit hyperactivity disorder in children and adolescents. Paediatr. Drugs 11, 203–226 (2009).
8. Proal, E. et al. Brain Gray Matter Deficits at 33-Year Follow-Up in Adults with Attention-Deficit/Hyperactivity Disorder Established in Childhood. Arch. Gen. Psychiatry 68, 1122–1134 (2011).
9. Wolosin, S. M., Richardson, M. E., Hennessey, J. G., Denckla, M. B. & Mostofsky, S. H. Abnormal cerebral cortex structure in children with ADHD. Hum. Brain Mapp. 30, 175–184 (2007).
10. Shaw, P. et al. Attention-deficit/hyperactivity disorder is characterized by a delay in cortical maturation. Proc. Natl. Acad. Sci. U. S. A. 104, 19649–19654 (2007).
11. Webb, J. T., Amend, E. R. & Webb, N. E. Misdiagnosis and Dual Diagnoses of Gifted Children and Adults: ADHD, Bipolar, OCD, Asperger’s, Depression, and Other Disorders. (Great Potential Press, 2005).

Leave a comment